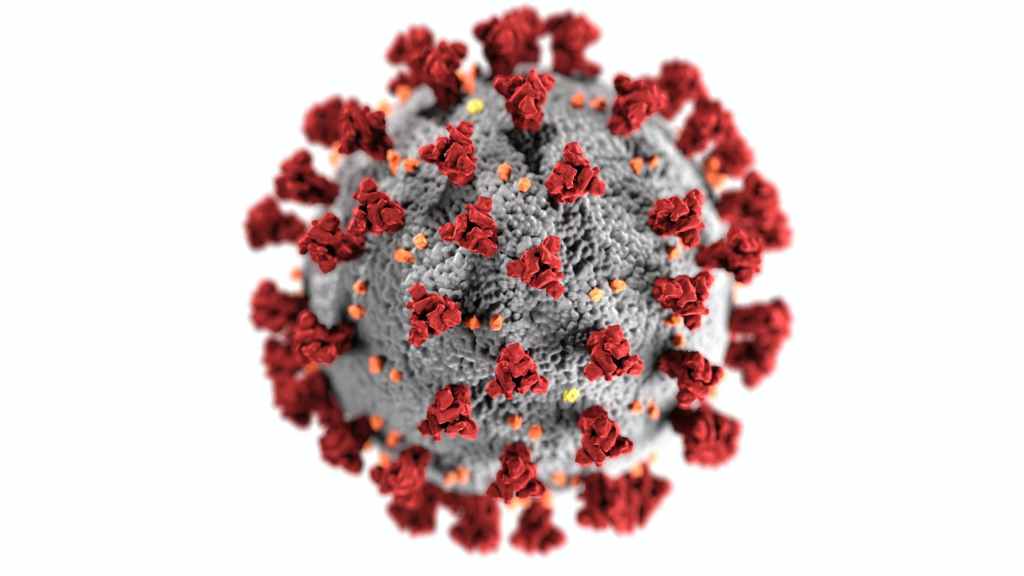
इस लेख में हम लोग डेल्टाक्रोंन वॉयरस के विषय में होने वाली आवश्यक जानकारी प्राप्त करेंगे | इसके विषय की जानकारी रहने पर हम लोग अपने को एवं अन्य लोगों की जान बचा सकते है |
जब दो तरह के वायरस एक साथ एक ही मरीज को संक्रमित करते है तो उनके बीच म्युटेशन का आदान प्रदान होता है और वायरस का एक नया प्रजाति उत्पन हो सकता है|
बहुत मरीज डेल्टा एवं ओमीक्रॉन से एक साथ संक्रमित होते है | जब दोनों एक साथ एक मरीज को संक्रमित करते है तो उनके बीच म्युटेशन का आदान प्रदान हो सकता है और वायरस का एक नया प्रजाति उतपन्न हो सकता है |
डेल्टाक्रोंन क्या है ?कैसे नाम हुआ |
सायप्रस एक यूरोपीय देश है| सायप्रस विश्वविद्यालय के प्रोफेसर ‘ ‘ल्योनडीस कोस्टरीकिस ‘ और उनकी टीम ने अस्पताल में भर्ती २५ कोविड -१९ के मरीजों के सैंपल के जाँच में डेल्टा जीनोम में ओमीक्रॉन का जेनिटिक सिग्नेचर पाया | जिसके आधार पर इसे डेल्टाक्रोंन का नाम दिया है | यह कोविड -१९ के मरीज जो अस्पताल में भर्ती नहीं है उसमे नहीं पाया गया | इन सैंपलों को जाँच करने हेतु सात जनवरी को GISAID ,( इंटरनॅशनल डाटाबेश जो वायरस म्युटेशन का अध्ययन करता है ) भेजा गया है ,जिसका रिपोर्ट आना शेष है |
सायप्रस के हेल्थ मंत्री ने भी इस पर विश्वाश नहीं किया है और कुछ दिनों में इसके विषय में आधिकारिक वक्तव्य देने का आश्वासन दिया है |
अभी तक सभी विशेषज्ञो और बैज्ञानिकों का मानना है की ऐसा लैब के गलती से हुआ होगा | लैब में ऐसी गलतियां हो जाया करती है | ग्लोबल हेल्थ के विशेषज्ञ ‘वोघुमा कबेसिन तीतनजी’ ,डॉक्टर जेफ्री बैरेट और अन्य विशेषज्ञो और बैज्ञानिकों ने भी इसे लैब कंटैमिनेशन माना है |
डेल्टाक्रोंन के लक्षण
अभी इसकी पुस्टि नहीं हुई है ,अतः यह अनुमान लगाना ही गलत होगा कि इसके क्या लक्षण होंगे |
डेल्टाक्रोंन की अभी पुस्टि नहीं हुई है | कोवीड -१९ के रोकथाम के लिए उठाए जाने वाले सभी कार्य करना है | कोवीड -१९ के रोकथाम के लिए उठाए जाने वाले कार्य
१. बार बार साबुन पानी से हाथ धोना है | अगर साबुन पानी उपलब्ध नहीं हो तो अलकोहल वाले सांइटिज़ेर का इस्तेमाल बार बार करना है | चेहरे को कम से कम हाथ से छूना है |
२. आपस में छ फिट की दुरी रखना -सामाजिक दुरी का पालन करना जरुरी है |
३. चेहरे पर ठीक से मास्क लगाकर रहना है | खास कर जब घर से बाहर जाना हो तब मास्क लगाकर रहना है |
४. भीड़ वाले जगह पर जाने से परहेज करना है |
५. सरकारी नियमों का पालन करना है |
कोवीड -१९ का भविष्य
कोवीड -१९ का अभी और म्युटेशन आ सकता है | ओमीक्रॉन ही इसका अंतिम म्युटेशन का स्वरुप नहीं है | सभी विशेषज्ञो और बैज्ञानिकों का मानना है की कोवीड -१९ के म्युटेशन को रोकने के लिए ग्लोबल टीकाकरण (वैक्सीन )बहुत ही जरुरी है |
इस लेख में हम लोग H3 N2 इन्फ्लुएंजा वॉयरस के विषय में होने वाली आवश्यक जानकारी प्राप्त करेंगे | इसके विषय की जानकारी रहने पर हम लोग अपने को एवं अन्य लोगों की जान बचा सकते है |
H3 N2 Influenza virus A का एक सब टाइप है | यह वायरस’ ोरथोमिक्सोविरिडा’ ‘orthomyxoviridae’ family का है | इसका वैज्ञानिक नाम Influenza virus A सब टाइप H3 N2 है |
इसका नामकरण वायरस के बाहरी सतह पर मौजुद दो तरह के प्रोटीन -Hemagglutinin ((H ) एवं न्यूरोअमीनिडसे neuroaminidase (N ) के कारण किया गया है |
H3 N2 Influenza virus अन्य इन्फ्लुएंजा वॉयरस H 1 N 1 / H 1 N २ इत्यादि से ज्यादा संक्रामक है | H3 N2 Influenza virus में हर साल कुछ परिवर्तन होता है | इस वर्ष भारतवर्ष में H3 N2 Influenza virus के मामले में अचानक बहुत वृद्धि हुई है |
संक्रमण कैसे होता है
H3 N2 वायरस का संक्रमण सांस के द्वारा होती है। खांसी एवं सांस के द्वारा निकले बूंदो से यह वायरस फैलते है | यह संक्रमण सांस के द्वारा शरीर में प्रवेश करता है| इस वायरस का सबसे जरुरी बात यह है की यह सीधे LUNGS को संक्रमित करता है | और कोविड -१ ९ जैसे गंभीर गंभीर बिमारी के तरह हो जाती है |
H3 N2 वायरस संक्रमण के लक्षण :
इस H3 N2 वायरस के संक्रमण होने पर गले में खराश ,सर्दी खांसी ,नाक बहना , बुखार ,सर दर्द ,शरीर दर्द है| ज्यादा थकान ,छाती में दर्द ,पेट में दर्द ,जी मिचलाना ,उलटी और दस्त हो सकता है | ज्यादा होने पर या इम्युनिटी कम होने पर ऑक्सीजन की कमी हो जाती है SpO २ कम हो जाता है ९ ० से काम होने पर मरीज बेहोश हो सकता है | ऑक्सीजन से इलाज करना परता है |
बचाव :
सांस से सम्बंधित होने के कारण इसका प्रसार बहुत तेजी से होता है | इससे बचाव ही सवस्थ रहने का तरीका है | कोविड -१ ९ के समय किया गया उपाए अपनाना है :
संक्रमण को रोकने के लिए हर साल टीकाकरण कराना
भीड़ वाले जगह पे जाने से परहेज |
मास्क लागए ,दुरी बना कर रखें | अपनी हिफाजत करें और स्वस्थ रहें।
नियमित व्यायाम ,पौस्टिक भोजन
अपने हाथों को कुछ कुछ समय के अंतर से नियमित रूप से साफ करें। साबुन औरमरीज पानी का उपयोग करें,| अल्कोहॉल युक्त सैनीटाइज़र से हाथ रसाफ रखें ।
खांसने या छीकने पर अपनी नाक और मुह को अपनी कोहनी या रुमाल से ढक लें।बीमारी के लक्छन होने पर घर पर रहेंऔर आराम करें| अन्य लोगों से दुरी बनाकर रहना | अपने से दवा का सेवन न करें |
सावधानी :-
गर्भबती महिलाओं ,बच्चों और बुजुर्गों को खास सावधानी बरतनी है| कसी भी तरह का लक्षण होने से तुरंत स्वस्थय केंद्र जाएंऔर अपना अच्छे से जांच करवाएं।
पहले से बीमार ,दिल ,किडनी ,कैंसर के के मरीज ज्यादा सावधान रहे।
उपचार:- लक्षण होने पर तुरंत नजदीकी अस्पताल जाकर इलाज कराना चाहिए |
HASHTAGS : SpO २ #कोविड -१ ९ #नियमित व्यायाम #मास्क #टीकाकरण#सैनीटाइज़र#
मान्यता है कि पृथ्वी पर संकट होने भगवान विष्णु अवतार लेकर पृथ्वी परआये संकट को दूर करते हैं |भगवान विष्णु ने अनेक वार पृथ्वी परअवतार ले कर पृथ्वी को संकट से बचा लिया है| श्रीमद्भागवत पुराण में २२ अवतार का उल्लेख है]कुछ धर्मशास्त्रों में २४ अवतार का वर्णन है | जिसमे २३ अवतार हो चुके है और २४ वॉ अवतार कल्प अवतार होना बाकि है|इन में से दस अवतार मुख्य अवतार है]इसे दशावतार कहतें है |गरुड़ पुराण में दशावतार का वर्णन है |
१० क्लिकअवतार –मान्यता है की कलुयग के अंतिम चरण में इनका अवतार होगा
इनके आलावा विष्णु भगवान के अवतार|
११ श्री सनकादि मुनि अवतार |
१२ नारद अवतार|
१३ नर नारायण अवतार|
१४ कपिल मुनि अवतार |
१५ दत्तात्रेया अवतार |
१६ यज्ञ अवतार|
१७ ऋषभ देव अवतार|
१८ आदिराज पृथु अवतार|
१९ धन्वंतरि अवतार
२० मोहनी अवतार |
२१ हयग्रीव अवतार|
२२ श्रीहरि अवतार|
२३ वेदव्यास अवतार|
२४ हंस अवतार |
अवतार के विषय में विशेष जानकारी दूसरे लेख में प्राप्त करेंगे
अस्वीकरण : इस आलेख में व्यक्त किए गए विचार विभिन्न लेखों संचार माध्यमों से लिए गए है और सभी सूचनाएँ मूल रुप से प्रस्तुत की गईं है| व्यक्त किए गए विचार लेखक के निजी विचार नहीं हैं तथा इसके लिए किसी भी प्रकार से उत्तरदायी नहीं है | मानवीय भूल टंकण भूल भी हो सकता है इसके लिए लेखक किसी भी प्रकार से उत्तरदायी नहीं है|
Introduction: The effects of exercise on the muscular system are of two types: Short-term and long-term results.
Keywords: Creatine phosphate |red muscles|type II or white muscles| Sympathetic vasoconstrictor |Sympathetic vasodilator| Anaerobic glycolysis|aerobic glycolysis|
Table of contents
1.
Short term effects
2.
Long term effects
3.
The blood supply in muscles
4.
Source of energy
5.
Summary
A. Short-term effects of exercise:
1. Exercise increases blood supply, especially in the exercising muscles. During exercise, the metabolic demand of muscles increases, and metabolic waste product also increases. As a result, the supply to the exercising muscles increases to meet these demands and to remove waste.
Blood supply to the muscles:
Normal blood supply is 3-4 ml/100gm/minute. In an average adult male of 70 kg, the weight of muscle is about 30 kg. So 300 x3=900 ml/minute. It may increase to 100 ml/100 gm/minute,i.e.,300x 100=30000. 1 kg=1000gm.30×1000=30000gm.
100 gm—4 ml, so 30000gm — 4x 30000/100=300 x 3=900ml, and in strenuous exercise, it may increase (30000×100/100=30000=30 liters/minute) up to 30 liters per minute. This indicates that vascular resistance is very high in muscles in resting muscles.
3/4th of total body muscles is of type II or white muscle. They are responsible for short, muscular activities. These muscles suffer from oxygen debt.
Rest 1/4th is the type I or red muscles responsible for posture maintenance. They consume less volume of oxygen and are unlikely to develop oxygen debt.
Total peripheral resistance is mainly due to the resistance of vessels of muscle.
The basal myogenic tone of the pre-capillary resistance vessels is responsible for the resistance.
Sympathetic vasoconstrictor (that constrict blood vessels) nerves mainly control the basal myogenic tone of the pre-capillary resistance vessels. Therefore, impulses from these sympathetic vasoconstrictor nerves constrict the pre-capillary resistance vessels, decreasing the mean capillary pressure that increases the uptake of tissue fluid, and impulses from the sympathetic vasoconstrictor nerves constrict the post-capillary venules that push blood toward the heart.
Average, sympathetic discharge is one impulse /second in resting muscles. When sympathetic activity increases, hypotension can reduce muscle blood flow to 0.3 to 0.5 ml/minute/100 gm of muscles. In that condition, blood flows to vital organs.
When sympathetic activity decreases, the tone of the pre-capillary resistance vessels reduces, and muscle blood flow increases.
Increased body temperature inhibits the normal ‘bulbar vasomotor drive to the thoracolumbar sympathetic neurons. When the sympathetic impulse to the pre-capillary resistance vessels reduces, blood flow in the muscles increases. Likewise, body temperature rises in exercise, so muscle blood flow increases.
The sympathetic vasodilator nerves act on the arterioles only and dilate their arterioles. Dilatation of the arterioles reduces peripheral vascular resistance in the muscles. As a result, the sympathetic vasodilator nerves may increase muscle blood flow to 30-40 ml/100 grams /minute.
The cortico-hypothalamic-reticulo-spinal pathway controls the sympathetic vasodilator nerves. Stress, emotions, and the anterior hypothalamus affect the sympathetic vasodilator nerves. But the medullary afferents –chemoreceptor and baroreceptor fibers do not affect the sympathetic vasodilator nerves.
Psychicmusclevasodilation: before exercise starts, blood vessels in muscles dilate, increasing the blood supply in the muscles.
Chemical factors – During exercise, the following changes occur in the exercising muscles :
oxygen level decreases- hypoxia,
carbon dioxide level increases
potassium and hydrogen ions increase
All these changes cause vasodilation by local action on the pre-capillary resistance vessels and arterioles.
In addition, local metabolic product accumulation dilates arterioles and pre-capillary sphincters and increases the production and release of nitric oxide –a vasodilator.
Dilatation increases systolic blood pressure and hydrostatic pressure leading to an increase in filtration pressure. As a result, fluid from the capillaries enters into interstitial tissue, and plasma volume decreases. The fluid portion of blood decreases but cells and macromolecules remain the same, causing haemoconcentration, and hyperosmolality occurs at the interstitial tissue level. Blood flow increases through the muscular capillaries. Hyperosmolality reduces myogenic pacemaker activity and relaxes the vascular smooth muscles.
Compression of blood vessels during muscle contraction reduces blood supply in the muscle. Therefore, metabolic end products accumulate in the muscles, in addition to reducing oxygen supply.
Accumulation of metabolic end products irritates free nerve endings-causing pain and fatigue. During this period, myoglobin supplies oxygen. Myoglobin stores oxygen, which will supply oxygen only for 10 seconds during exercise. If the activity continues, anaerobic metabolism starts.
During muscle relaxation, pressure on the vessels is abolished, blood flow increases, and nutrients and oxygen supply resume. Creatine phosphate is restored. Myoglobin accepts oxygen and stores oxygen.
2. Exercise increases body as well as muscle temperature. Muscle efficiency during contraction is only about 25%.
Muscle activity uses energy. ATP is the only immediate source of energy. In a single muscle fiber, little ATP is stored, but creatine phosphate is stored in a large amount. When the ATP level falls, it is generated rapidly from ‘creatine phosphate’ until all the creatine phosphate is used. During rest or relaxation, creatine phosphate is formed in the mitochondria ( sarcosomes).
ADP + Creatine phosphate è ATP + Creatine
During rest, ATP is produced in the muscle cells. However, when energy from fuel is added to ADP, ATP is formed.
ADP + Pi + Food energy à ATP
In light exercise, ATP formation is due to the oxidation of glycogen and free fatty acids.
In moderate exercise, glycogen is also used along with free fatty acids. Glycogen stored in muscles and the liver dissociates into glucose by oxidation-aerobic glycolysis. Aerobic glycolysis produces 38 ATP, while free fatty acids produce 147 ATP.
In severe exercise, aerobic glycolysis fails to provide energy, so other methods come into the scene:
1. Anaerobic glycolysis occurs (glycogen is broken down without oxygen), which produces 2 ATP molecules from one glucose molecule.
In isotonic contraction, about 25% of the energy utilized by the muscle performs work, and the rest, 75%, convert into heat.
In isometric contraction, no work is performed, and 100% of the energy is converted into heat.
Exercise decreases muscle viscosity, therefore, increases muscle flexibility. In addition, blood circulation increases before the activity start due to psychic stimulation.
4. Micro tears in muscle fibers occur during exercise, which is responsible for delayed onset muscle soreness.
5. Lactic acid accumulation stimulates free nerve endings leading to pain. In addition, it inhibits ATP generation within the muscle.
Lactic acid is used by other muscles or body tissue as a source of energy. In the liver, lactic acid is transformed into pyruvate, which is used to form ATP.
B. Long-term effects of regular exercise:
Hypertrophy (size) and hyperplasia (increase in muscle fiber number) of muscles occur.
2. Existing capillaries in the muscles open, and new capillaries and collateral vessels develop in the muscles to increase blood supply.
3. Strengthen tendons and ligaments
4. Mitochondria, myoglobin increases in number and size.
5. In the muscles, glycogen storage and enzymes used in glycogen metabolism increase.
6. Lactic acid tolerance increases.
7. Increase in oxidation metabolism.
8. Improve reaction time and delay fatigue.
Exercise is beneficial for muscles,and the heart.
Summary:
Short-term effects:
Increases blood supply to the muscles and body
Increases activity of muscle fibers
Long-term effects:
Hypertrophy and hyperplasia
Increases muscles, tendons, ligaments, heart, and respiratory system power.
About’ totalphysiology.com.’ and learn-and-fly. co. in.’
This article is part of my mission to provide trustworthy recent health information to support the general public, patients, and professionals globally. Here you will find human Physiology, Anatomy, and health-related topics.
Acid-base disturbance
The acidity or alkalinity of any solution is indicated on the ph scale.
The ph scale is from ‘0’ [strongly acidic]to 14[strongly alkaline].
The proper pH of the human body is maintained at a very constant level that is between 7.35 to 7.45. Therefore, a narrow range of pH is essential for normal physiological functions.
A chemical system that resists change in the fluid Ph is a buffer system.
The body buffers, kidneys, and respiratory system mainly maintain body pH.
The primary buffers in the body fluids are:
1. Bicarbonate buffer system
2. Hemoglobin buffer systems
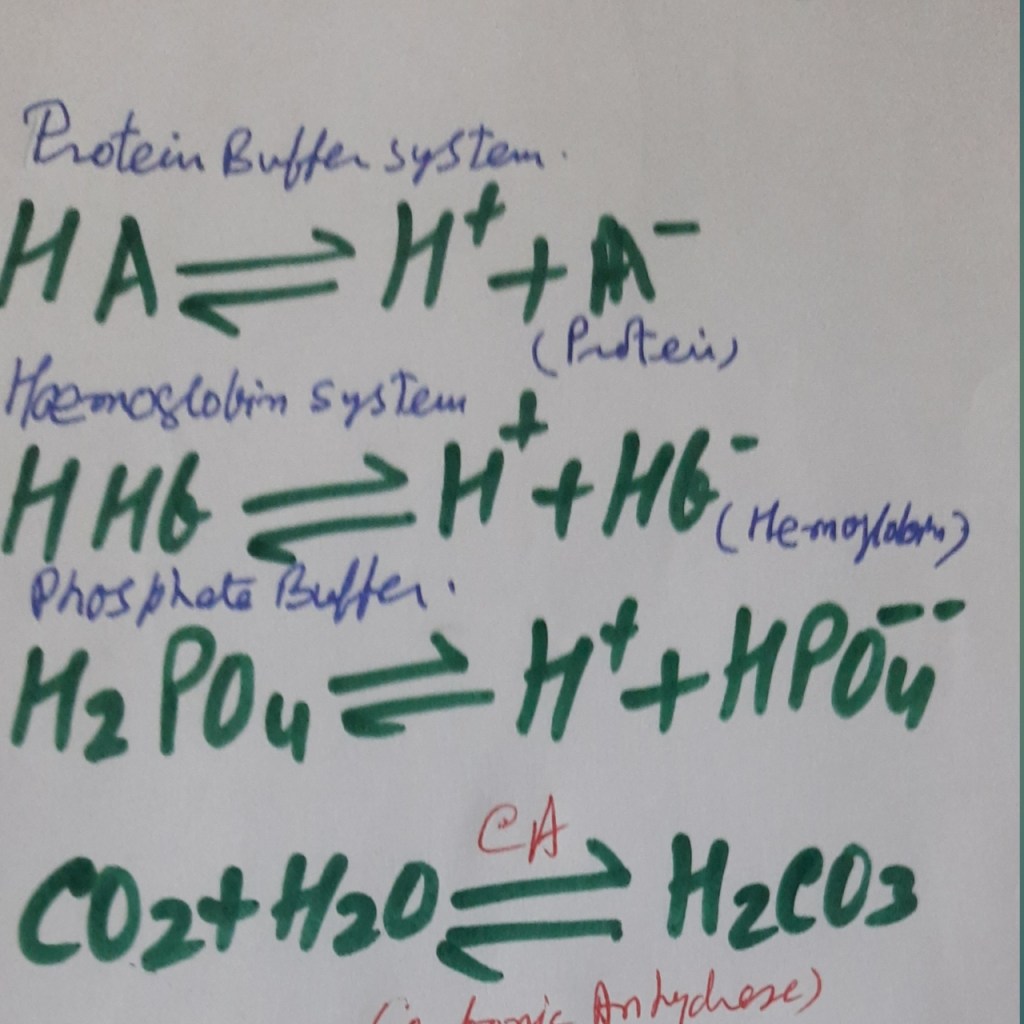
3. Protein buffer systems, and
4. Phosphate buffer systems.
The respiratory system rapidly(minutes) adjusts the blood pH, while the renal system adjusts blood pH slowly (hours to days)by excretion of H+ ions and conservation of bicarbonate.
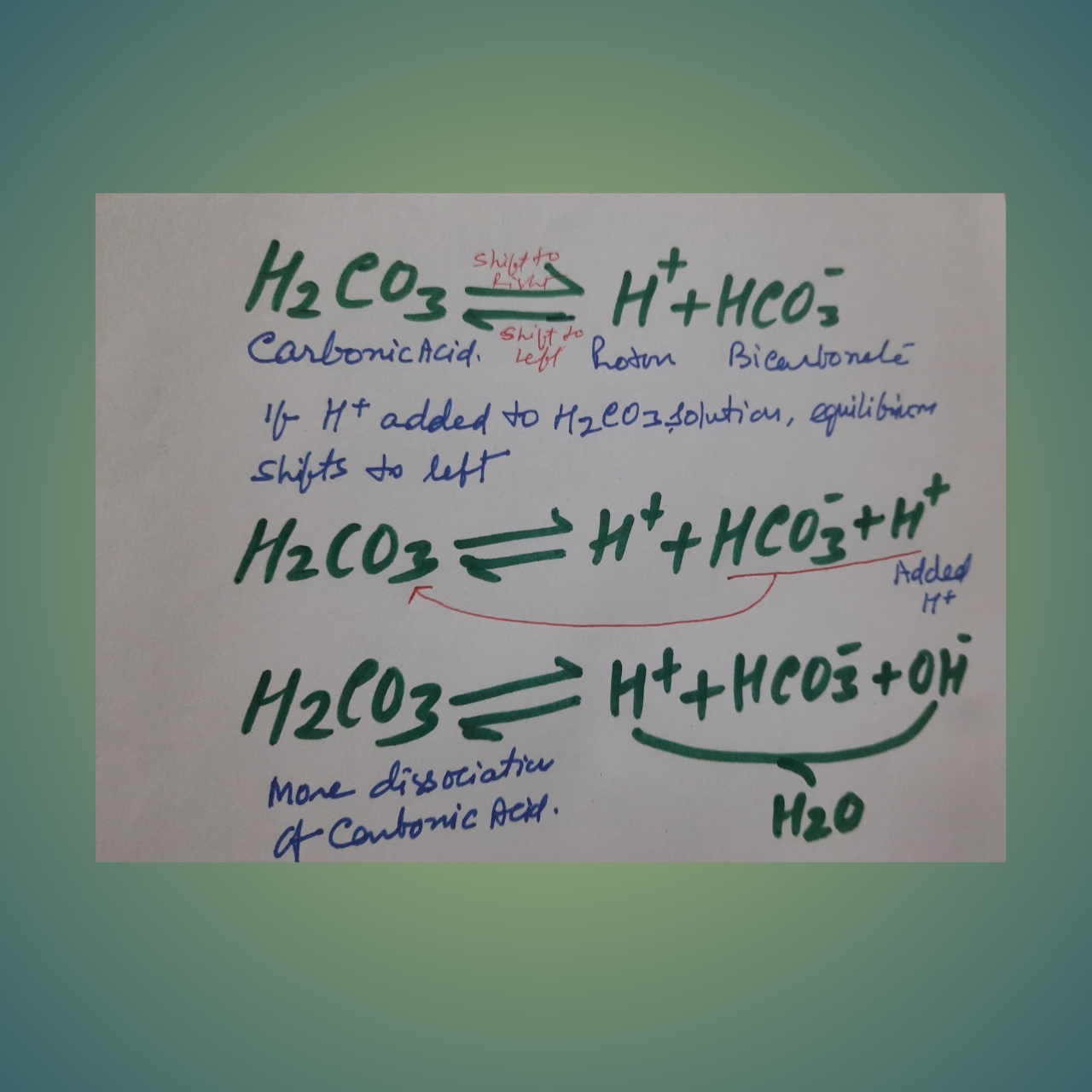
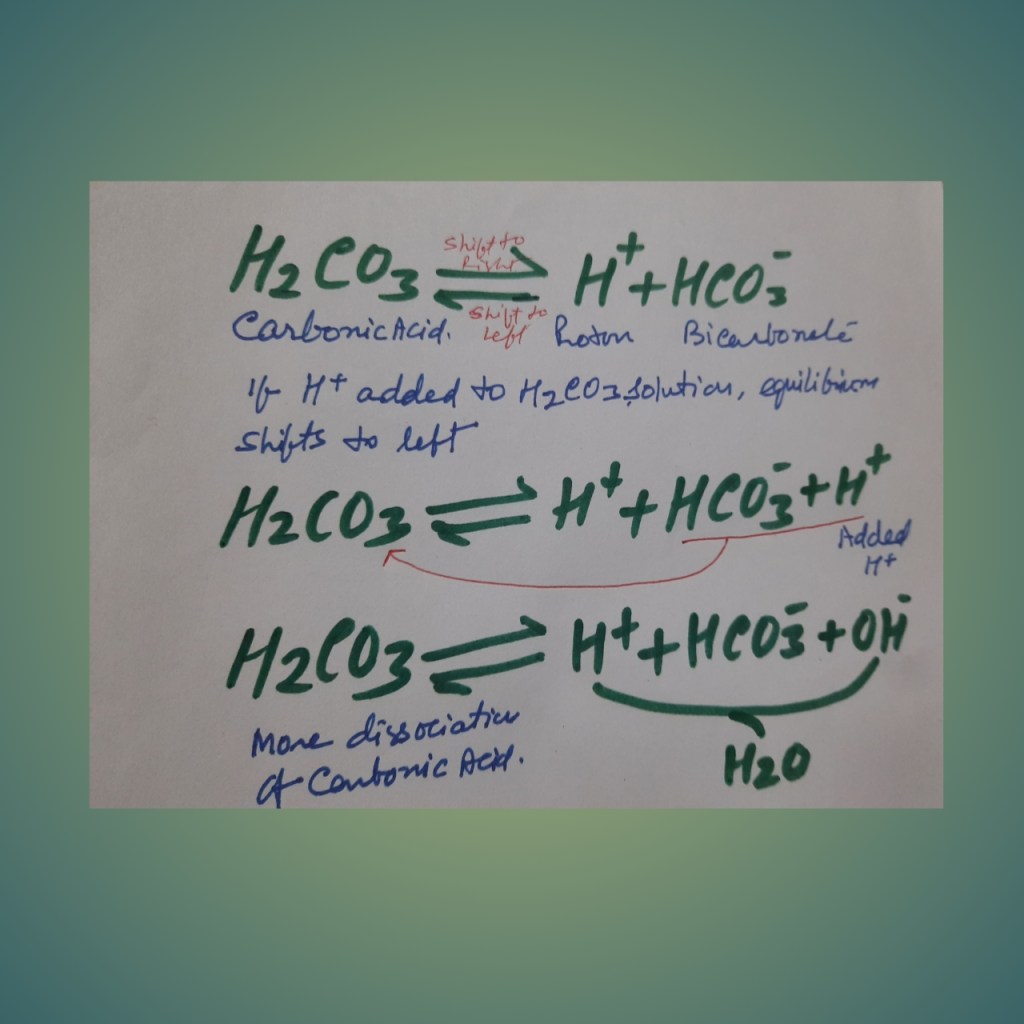
Bicarbonate buffer system= carbonic acid-bicarbonate system: In this system, Carbonic acid (a weak acid), along with its conjugate base, is present. Carbonic acid is a weak acid and dissociates into hydrogen and bicarbonate ions.
If a powerful acid is added to the solution with the bicarbonate buffer system, more hydrogen ions are added, then the equilibrium shifts to the left. Most of the added hydrogen is removed from the solution maintaining the Ph.
If a base (hydroxyl ion) is added, hydrogen and hydroxyl ions will form water and remove the hydrogen ion from the solution, that decrease [H + ]. As a result, more carbonic acid dissociates, and the decline in hydrogen ion concentration is minimized.
The carbonic acid bicarbonate system is a very effective buffer system in the body due to the:
1. The bicarbonate level in plasma is in equilibrium with the dissolved carbon dioxide controlled by respiration.
2. The Kidneys regulate the plasma concentration of bicarbonate.
The bicarbonate buffer system is rapid as it depends on respiration.
Hemoglobin – The hemoglobin buffer system is responsible for 90% of the buffering capacity for carbonic acid. Red blood cells contain hemoglobin.
The buffering action of hemoglobin is due to imidazole groups of the histidine residues-38 histidines in one hemoglobin molecule.
Deoxy hemoglobin or reduced hemoglobin is a more effective buffer.
Hydrogen ions produced by CO2+H 2O àH 2CO3+ H+ are buffered by hemoglobin, which is reduced by oxygen dissociation.
Protein buffer systems-.
Proteins are amphoteric -behave as acids or bases according to the body’s conditions. At average pH (7.4) plasma proteins are ionized-
C terminal end is the form of COO–, will bind with any added acid while
The N-terminal end is as NH3+ that binds with any added alkali.
All proteins are buffers and function mainly intracellular. Therefore, it is responsible for all intracellularly buffering action and about 2/3 of the buffering power of the blood.
Amino acids form proteins. They contain positively charged amino groups and negatively charged carboxyl groups.
The charged groups bind hydrogen and hydroxyl ions and thus work as buffers.
Phosphate buffer system:
The phosphate concentration is low in plasma, so their buffering power is less. But phosphate compounds are abundant in the intracellular fluid, therefore an important intracellularly.
When the carbonic anhydrase enzyme is absent (for example, there is no carbonic anhydrase in plasma.) reaction of carbon dioxide and water to form bicarbonate proceeds slowly in either direction.
When the enzyme is present (an abundant amount in RBC, Gastric acid secretion cells, and Renal tubular cells), the reaction of carbon dioxide and water forms bicarbonate which proceeds swiftly in either direction.
Acidosis or acidemia is an abnormal condition in which the acid content in the human body is high. An increase in the hydrogen ion concentration
decrease in pH value.
Acidosis is of two types-
Metabolic acidosis ,and Respiratory acidosis.
Alkalosisor alkalemia is a clinical condition due to excessive accumulation of base or loss of acid, sufficient to increase pH level above normal.
Types of alkalosis:
Metabolic alkalosis and Respiratory alkalosis.
Acidosis is due to
a] increase in hydrogen [acidic compounds-due to1.exogenous-increased intake 2. Endogenous-increased production in the body and reduced elimination.
B] decreased base in the body
Low intake- exogenous,
Decreased formation and increased elimination.
Alkalemia is due to
Increase in the level of base:
1. Exogenous-increased intake 2. Endogenous-increased production in the body and reduced elimination and,
B] Decreased level of acid in the body
Low intake- exogenous,
Decreased formation and increased elimination.
Role of Kidneys
Kidneys will increase the excretion of hydrogen ions and increase the absorption of bicarbonates to maintain body pH. This is a slow process.
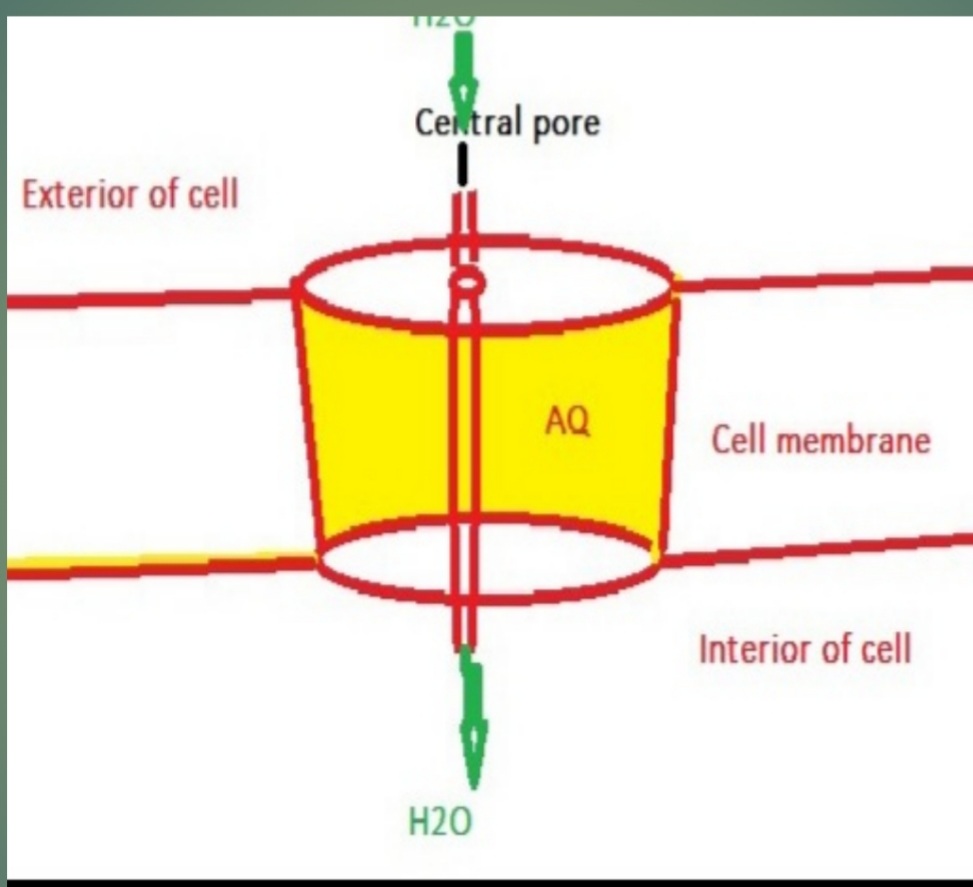
Aquaporins are integral cell membrane proteins that perform like channels for water and, in some cases, tiny solute molecules across the cell membrane.
Types and location:
In humans, about twelve aquaporins are detected. They are located in different types of cells. Their locations are :
Sr.no.
Type of Aquaporin
Cells and organs’ location
1.
AQ 0
Lens
2.
AQ 1
Blood vessels, eye, ear, and Proximal convoluted tubule
3.
AQ 2
Distal convoluted tubule, P-cells of collecting duct of the renal tubule.
4.
AQ 3
P-cells of collecting duct, Respiratory, urinary and digestive systems.
5.
AQ 4
Basolateral part of the plasma membrane of P-cells of collecting duct of the renal tubule.brain astrocytes, eye, ear, Skelton muscles, and parietal cells of the stomach.
6.
AQ 5
In the secretory cells of salivary, salivary, and sweat glands.They are also present in ears, and eyes.
7.
AQ 6
Intracellular vesicles in ‘I -cells’ of the renal tubule collecting duct.
8.
AQ 7
In brush borders of proximal convoluted tubular cells, kidneys, adipose tissues, and testis.
9.
AQ 8
In the proximal convoluted tubule, Intracellular in the liver, kidneys, and testis.
10.
AQ 9
In liver and leucocytes
11.
AQ 10
In the intestine.
Table describing types of aquaporins and organs where they are present
Some aquaporins are also present in the bones, spleen, and lungs.
Aquaporins perform essential and specific functions in each organ.
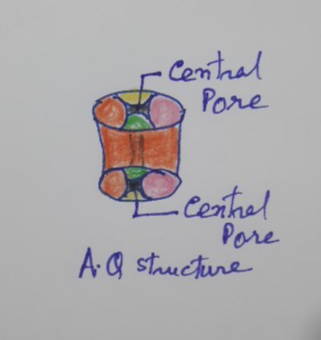
Structure of aquaporins :
Aquaporins are protein molecules with a pore in the center.
Mechanism of functions:
The kidneys regulate pore size by the ‘Antidiuretic hormone. Under the influence of ADH size of pores increases leading to increased water absorption.https://amzn.to/3tEtIyO
Functions :
The primary function of Aquaporin is to provide channels for water absorption. Therefore, aquaporins are very important for water balance in humans. For example, mutations in aquaporin 2, present in P- cells of the collecting duct of the renal tubule, result in diabetes -insipidus.
Diabetes insipidus is characterized by increased output of diluted urine -about 20 liters or more in a day. Recall that the average urine output is only 1.2 -1.5 liters per day.
Diabetes insipidus is due to a deficiency of ADH hormone, whereas Diabetes mellitus is due to insulin deficiency. In Diabetes mellitus, urine contains glucose, and its specific gravity is more than usual.
AQUAPORIN STRUCTURE WITH A CENTRAL PORE
Aquaporin in the cell membrane. Aquaporin has a central pore through which water passes.ADH regulated the size of the pore.
This article is part of my mission to provide trustworthy recent health information to support the general public, patients, and professionals globally. Here you will find human Physiology, Anatomy, and health-related topics.
Introduction
Thalassemia is a congenital blood disorder due to a defect in hemoglobin synthesis. Due to abnormal hemoglobin, red blood cells are destroyed prematurely, leading to anemia. Thalassemia was first used in 1932. Before that, it was known as Mediterranean anemia. As the disease was first recognized around the Mediterranean sea.
World thalassemia day is May 8.
According to the ICD classification, thalassemia is D-56.
Β major-thalassemia is also known as Cooley anemia.
The genes are responsible for healthy hemoglobin production. The beta globin chain is encoded by a single gene on the short arm of chromosome11, while the alpha chain encodes two closely linked genes on the short arm of chromosome 16. Each cell contains four copies of the alpha globin gene, and each gene produces one-fourth of the alpha gene.
Normal HbA has gene αα/ αα
silent carrier of α-thalassemia has gene – α /αα
Mild thalassemia has –/αα gene
Major has – – / – α gene
Barts hydrops fetalis, all four genes are absent, so α chains are not produced; only beta chains are formed. Beta chains group in four; this is hemoglobin H (HbH).
Two alpha and two beta chains are present in adult hemoglobin (HbA). Two alpha and delta chains are present in adult hemoglobin (HbA2). Two alpha and two gamma chains are in fetal hemoglobin (HbF).
Normal HbA has 2 alpha and 2 beta chains. Alpha globin protein level equals beta globin protein level.
HbF has 2 alpha and 2 gamma chains, while HbA2 has 2 alpha and 2 delta chains. A single gene on chromosome11 encodes for beta, gamma, delta, and other chains.
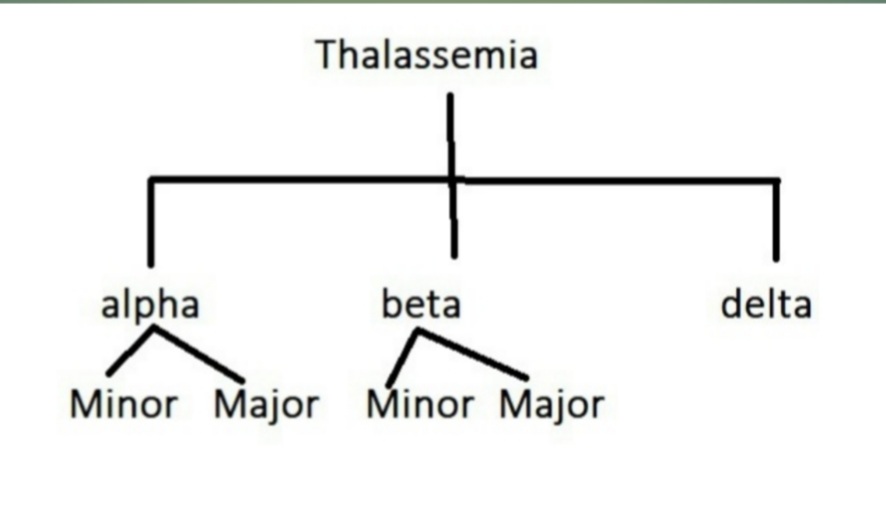
Types of thalassemia
Types of ThalassemiaThis Photo is by Sandhya Prasad, Licensed under CCBY.
Depending on the presence of a defect in the globin chain of the hemoglobin, thalassemia is classified as
α -thalassemia -the fault is in the α chain of the hemoglobin. When α-chain is absent, it is known as α – major thalassemia; when reduced, it is α -minor thalassemia.
2. β thalassemia -the defect is in the β -chain of the hemoglobin. When β -the chain is absent, it is known as β-major thalassemia, and when reduced, it is β -minor thalassemia. Intermediate beta thalassemia is also present. The beta globin chain is encoded by a single gene on the short arm of chromosome11. Each cell contains two copies of the beta-globin chain. The beta globin chain is encoded by a single gene on the short arm of chromosome11. β gene also codes for the gamma chain. Therefore,β-thalassemia is not apparent up to eighteen months of age due to fetal hemoglobin. An excess of α chains causes unpaired α-chains.
The beta globin chain is encoded by a single gene on the short arm of chromosome11,
The beta globin chain is encoded by a single gene on the short arm of chromosome11; β-major thalassemia is the most common type of thalassemia.
In normal HbA, b/b genes are present. In minor β- thalassemia b /- (one gene is present, another is absent, while in major -/-, no genes are present on the short arms of chromosome 11.
3. Delta thalassemia is also present as 3% of adult hemoglobin (HbA2) has a delta chain instead of a beta chain. Therefore, gene mutation to produce delta chains is responsible for delta thalassemia.
Thalassemia may coexist with other defects of hemoglobin. For example, it may coexist with sickle cell disease or sickle cell trait.
Thalassemia protects against malaria to some extent.
Incidence: About 280 million people were suffering globally, of which 4.4 lakhs were seriously ill—in 2015. About 7% of the world’s population is suffering from thalassemia. Incidence in India is about one million cases.
Thalassemia is very common in Italy, Greece, South Asia, the middle east, and Africa.
Sex : males: females ratio is 1:1(similar disease rates.).
The life span of an adult red blood cell is 120 days. However, in infants, the life span of red blood cells is less than 100 days.
About 2.4 million new erythrocytes are formed per second in humans.
Diagnosis:
History – Family history, history of blood transfusion, failure to thrive, and lethargy.
Physical examination: In mild cases, history will suggest the diagnosis; otherwise, one may miss the diagnosis.
The red blood cell has some enzymes for glycolysis and hexose monophosphate shunt to get energy.
Signs and symptoms:
In mild thalassemia, there are no symptoms. This may start insidiously. However, symptoms may be severe even to endanger life.
There is mild to severe anemia. Initially, signs and symptoms are due to anemia.
Signs and symptoms of anemia:
If anemia is mild, there is no sign and symptoms, and it goes unnoticed. But when anemia worsens, the symptoms appear and intensify. The symptoms are not specific and include:
1. Lethargy, extreme fatigue.
2. Weakness.
3. Chest pain
4. Headache, dizziness, or lightheadedness
5. Brittle nails
6. Pale skin, palm.
7. Poor appetite
8. Soreness of tongue
Signs are :
Pale skin, in severe cases person, will become paperwhite.
In an early case of anemia, examining the color of the lower conjunctiva and the palm will reveal that they are pale.
Abdomen examination: splenomegaly(enlarged spleen) may be present.
Excessive iron accumulates in the body due to the rapid destruction of red blood cells and frequent blood transfusions. In thalassemia, iron deposits in the liver, heart, and other systems, including the endocrine system. This iron deposit damages the functions of these tissues and may be fatal. Therefore, the iron chelating agent is given to remove irons from the tissues.
Excessive red blood cell formation results in abnormal bone structure, especially in the face and skull. As a result, bone marrow expands, and the bone becomes brittle and may fracture easily. Maxillary overgrowth (chipmunk ), malocclusion of teeth, frontal bossing, chronic sinusitis.
X-ray skull shows generalized skeletal osteoporosis, hair on end appearance.
X-ray ribs, vertebrae, metacarpal bones, etc., shows thinning of the cortex. Therefore, bones become brittle.
The spleen enlarges due to the destruction of red blood cells. An enlarged spleen makes anemia worsen.
Cardiac problems may lead to heart failure and abnormal cardiac rhythm.
Increased incidence of infection occurs in thalassemia.
In thalassemia, the growth rate decreases, which is apparent in children. This is due to defective secretion of growth hormone.
In suspected cases, prenatal testing may diagnose the condition.
Diagnosis of thalassemia is confirmed by complete blood count, special hemoglobin investigation-electrophoresis, high-performance liquid chromatography, and genetic test. Serum ferritin, red cell phenotyping, DNA analysis, and LFT are diagnostic tools.
Complete blood count -Microcytic (small red blood cells), hypochromic RBC.Microcytosis without an increase in RDW.
Peripheral blood film examination shows reticulocytosis.
Osmotic fragility decreases. The urine investigation shows increased urobilinogen.
Mentzer index indicates thalassemia. It is calculated from the complete blood count. It is MCV( mean corpuscular volume) per red cell count. If it is less than 13, it suggests a thalassemia trait. And if the value is more than 13, it is due to iron deficiency anemia.
Rapid hemolysis and repeated blood transfusion cause iron accumulation in different organs and affect their functions. Iron is deposited in the liver, heart, endocrine glands, etc. Features of hypothyroidism, hypoparathyroidism, hypopituitarism and insulin deficiency occur.
Complications of repeated blood transfusions, for example, infections of Hepatitis B, C, D, parvovirus B19, etc.
Prevention is better than cure; therefore, it is recommended that all couples must be tested for thalassemia -genetic testing and counseling.
Treatment: Medical treatment is not essential in mild thalassemia. In severe disease:
Repeated blood transfusion, iron chelation, and folic acid are the mainstay of treatment.
Indication of blood transfusion -Blood transfusion is given when Hemoglobin finding is below 7 gm /dl in two tests performed two weeks apart. Blood transfusion is given at an interval of four weeks to maintain hemoglobin at 9-10 gm/dl, and post transfusional hemoglobin level is 13.5 to 15.5 gm/dl.
Growth hormone replacement therapy is helpful in the expected growth of children.
A bone marrow transplant may be done.
For iron chelation -deferoxamine, deferiprone ., etc. are used.
FDA-approved drug is Hydroxyurea. However, thalidomide is also effective and is used in combination with Hydroxyurea.
Life expectancy is 50 -60 years in managed cases.
Cause of death -Congestive heart failure, arrhythmia, and /or multi-organ failure.
Summary
Thalassemia is not a curable disease, but treatment is available. Life expectancy is normal with proper treatment.
This article will be helpful for you.
Like to meet again? Sign up to get an email when I publish.
Andon’t’t forgets to follow me on learn and fly .co.in.
I am more enthusiastic, and you can get new insights from my articles later.
Thank you.
Disclaimer: All possible measures have been taken to ensure the accuracy and reliability of the information; however, ‘learn and fly.co.in’ does not take any liability for the same using any information provided by the website is solely at the viewers.’The information is provided as an educational service and public awareness. It is not medical advice.
In case of any medical health issue, we advise you to seek the advice of a qualified doctor and follow his instructions.
Progesterone is a steroid 21C, of course, endogenous in origin, and a progestogen sex hormone.
A progestogen is a group of steroid hormones. Progesterone is the main progestogen. The progestogen is an essential metabolic intermediate in synthesizing other endogenous steroids like sex hormones and corticosteroids.
Progestogen performs various functions as a neurosteroid essential for brain function.
Site of synthesis
Leading site
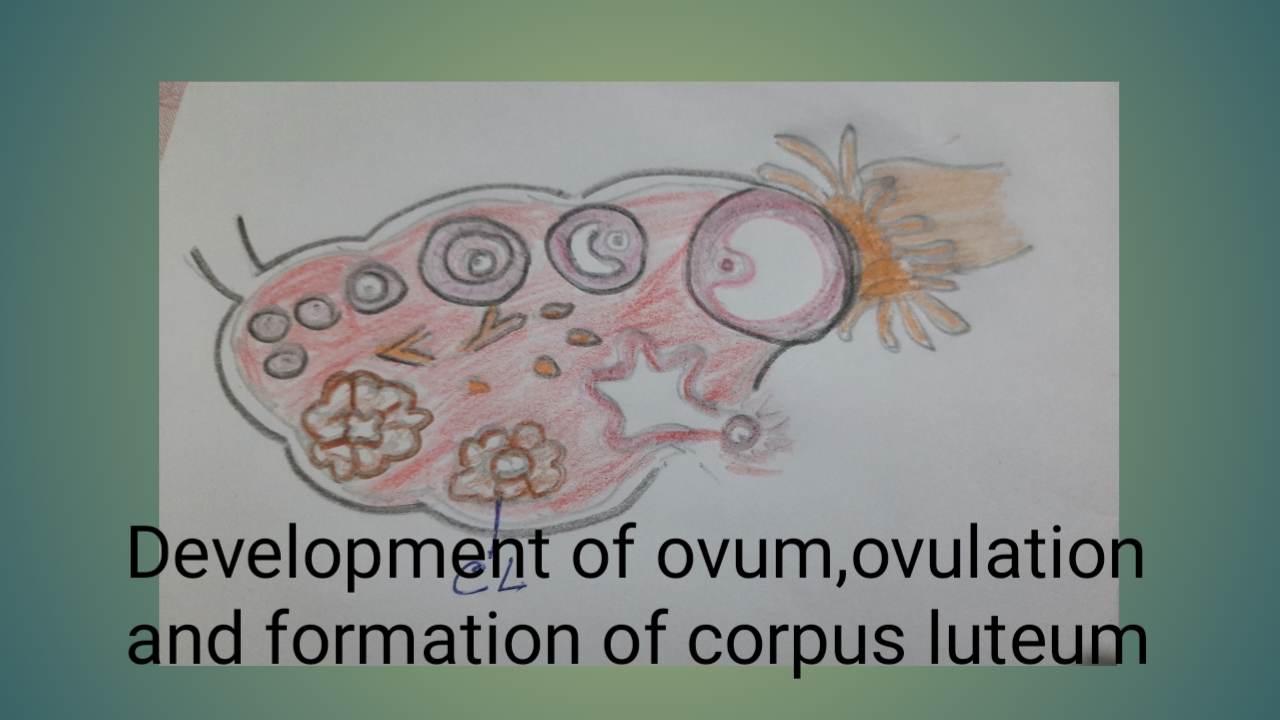
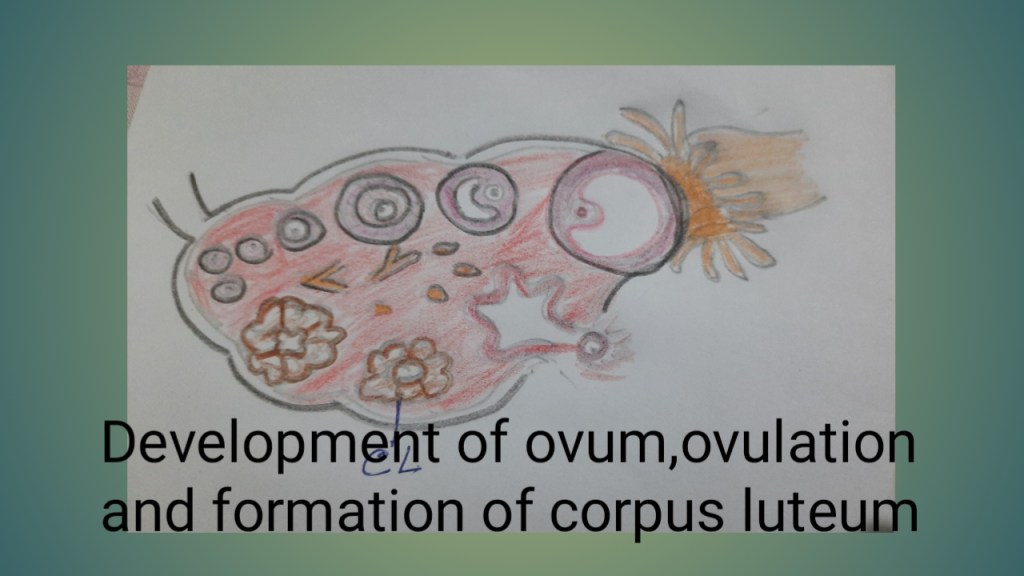
Progesterone is secreted mainly by “theca cells “of the corpus luteum and during pregnancy by the placenta in females. When ovulation fails, the corpus luteum is not formed. Therefore, progesterone synthesis will not take place. When pregnancy occurs up to six weeks, Progesterone is synthesized by the corpus luteum. The placenta synthesizes Progesterone and other hormones at six to eight weeks of pregnancy. This is known as the ‘luteal -placental shift.’ Syncytiotrophoblasts’ are the leading site of hormone secretion.
Photo by Sandhya Prasad
Minor sites
In small amounts, Progesterone is secreted from the adrenal gland in males and females.
Progesterone is also secreted to some amount in nervous tissues present in the brain and adipose tissues.
Animal source: Progesterone is present in milk products. Bioavailable progesterone level rises after the consumption of milk products.
Steps of Synthesis
The primary substrate is cholesterol. Cholesterol is oxidized to produce Pregnenolone.
The average level of Progesterone: progesterone levels are low in female children and postmenopausal women.
In females, its level fluctuates during the menstrual cycle. During the follicular phase of the menstrual cycle, progesterone level is 0.9 nanograms per milliliter, and during the luteal phase, it rises by 20-fold.
In late pregnancy, the average synthesis of Progesterone is 250 mg/day.
After delivery, plasma progesterone level decreases rapidly and is not detectable after 24 hours.
In males, progesterone levels are only 0.3 nanograms per milliliter.
Transport
Progesterone circulates in the blood in the free and bound stages.
80% Progesterone is bound to albumin
18% Progesterone is bound to ‘gonadotropin binding glycoprotein’ (GBG).
02% Progesterone is in the free state.
Functions of Progesterone
In conjunction with estrogen, Progesterone stimulates the uterus’s growth and secretory changes in the endometrium. It has no action of its own. The stroma cells proliferate. The spiral arteries grow, become more coiled, and dilate. The length and diameter of the endometrial glands increase and become tortuous.
It inhibits the contraction of the myometrium.
Progesterone, along with estrogen, causes the development of the lobuloalveolar system of the breast during pregnancy.
Progesterone increases Basal body temperature (BBT) to some extent. At the time of ovulation, BBT increases by 0.50 °C (0.9 °F).
Under the influence of Progesterone, cervical secretion becomes thick and tenacious.
Progesterone has an Immunomodulatory role by inhibiting T-lymphocyte-mediated tissue rejection and protecting the conceptus.
Progesterone stimulates the rate of respiration.
Progesterone inhibits ovulation. Progesterone à(-) GnRH release from hypothalamus à (-) LH.
Progesterone decreases the effects of estrogen by
1. reducing the number of estrogen receptors, and
2. converting potent estrogen to a less potent derivative.
A large dose blocks the action of aldosterone on the kidneys, leading to increased loss of sodium-natriuresis.
Progesterone decreases myometrial excitability by stabilizing lysosomal membranes and inhibiting prostaglandin synthesis.
Progesterone antagonizes the action of estrogen| the female sex hormone, during labor.
Metabolism
Progesterone is rapidly metabolized by the liver to pregnanediol. Though extra hepatic tissues like the brain and skin also metabolize Progesterone.
So, sites of metabolism – mainly hepatic, and to some extent, Extrahepatic.
The main metabolic pathway is reduction. And then, conjugation occurs in the liver.
This pregnanediol conjugates to glucuronic acid, which is water-soluble and excreted in the urine.
When given orally, it is metabolized rapidly; therefore, it is used parenterally. But synthesized Progesterone can be given orally.
Mechanism of Action
Progesterone is secreted in increasing amounts from the trophoblast of the placenta. The precursor of pregnenolone is maternal cholesterol. In the endoplasmic reticulum, pregnenolone is converted into Progesterone by 3-beta-hydroxysteroid hormones, which readily diffuse passively across the cell membrane. Progesterone, being a steroid hormone, rapidly diffuses across the cell membrane. Progesterone enters all cells, but it has action only when progesterone receptors (PR) are present. It exerts effects mainly on the ovary, uterus, and breast. This is due to the presence of ‘progesterone receptors.
Progesterone receptors (PR) are of two types:
Nuclear progesterone receptors (NPR) and membrane progesterone receptors (PR)
Progesterone receptor is expressed in specific tissues, including the ovary, uterus, and breast.
Nuclear Progesterone receptors (NPR): Progesterone binds to and activates progesterone receptors in the cytoplasm. The progesterone receptor is a dimeric nuclear protein. Progesterone with a ‘nuclear progesterone receptor’ forms a complex that attaches to a specific DNA sequence, activates the transcription of target genes, and promotes cell replication and protein synthesis. The DNA sequence is known as the ‘hormone response element.’ This initiates new messenger RNA that causes cell replication and protein synthesis.
Progesterone with a ‘membrane progesterone receptor (PR)’ regulates oocyte maturation, sperm motility, labor, and cancer.
Progesterone acts as a ligand of the progesterone receptor membrane component 1(PGRMC1) and regulates metabolic functions and neuron viability.
Regulation of Progesterone Secretion
Under the higher centers, the Hypothalamus secretes releasing hormone, GnRH, which induces the release of luteinizing hormone (LH) from the anterior pituitary gland.
Luteinizing hormone (LH) activates ‘adenyl-cyclase’ in the corpus luteum.
Due to ‘adenyl-cyclase,’ more cyclic AMP is formed, which induces progesterone synthesis.
It has a negative feedback effect on the release of GnRH from the hypothalamus.
Estrogen is the main female sex hormone that is secreted mainly from the ovaries. Chemically estrogens are steroids. Estrogens are secreted in all vertebrates and even in some arthropods.
Oestrogen -Estrone was isolated in 1929 for the first time.
Oestrogen originates from Ancient Greek ‘oestros’ ( a periodic state of sexual activity in female mammals) + ‘genos’ (generating). The term was used in 1920.
Site of estrogen synthesis:
Ovaries –
Cells of theca interna of the Graafian follicles are the primary site of estrogen secretion.
Granulosa cells of the Graafian follicles—secrete estrogen, which remains in the Graafian follicles.
Placenta during pregnancy
Adrenal cortex -in small amounts
Testis – in small quantities.
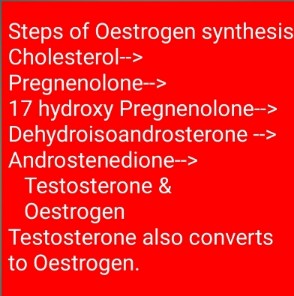
Synthesis of estrogen:
The primary substrate for steroid synthesis is cholesterol. Therefore, Oestrogen is also a steroid hormone synthesized from cholesterol.
ESTROGEN SYNTHESIS
Sources of cholesterol are
Acetate during the follicular phase, and
Low-density lipoprotein (LDL) during the luteal phase.
Also, uptake from the circulating blood.
Cholesterol is converted into Pregnenolone by the mitochondrial enzymes – cholesterol -desmolase in mitochondria of the theca interna cells. Cytochrome P450 family of enzymes in the mitochondria catalyze most steroidogenic cell reactions. Pregnenolone enters the endoplasmic reticulum (ER),
Where it is dehydrogenated by 3-beta hydroxysteroid dehydrogenase to form Progesterone
Progesterone is converted to 17-hydroxy Pregnenolone by 17-alpha hydroxylase.
17-alpha pregnenolone is converted into dehydroisoandrosterone (DHA).
Dehydroisoandrosterone (DHA) is converted in Androstenedione, which is converted mainly into Estrone, estradiol, and some testosterone. Testosterone and Androstenedione are aromatized under the influence of FSH to estrogens.
Control of secretion:
Two anterior pituitary gland hormones, FSH (Follicular stimulating hormone ) and LH( luteinizing hormone), contr̥ol estrogen secretion.
Effect on FSH:
Negative feedback: Oestrogen exerts negative feedback effects on FSH release by two direct methods: It reduces pituitary sensitivity to GnRH and decreases GnRH secretion, probably by decreasing dopaminergic activity.
Effect on LH:
In high concentrations, estrogen exerts a positive effect -increasing GnRH secretion from the hypothalamus and increasing sensitivity of the anterior pituitary to GnRH.
Daily secretion :
In females
1. During menstrual, daily secretion differs with two peaks phase.
One just before ovulation 200-500 microgram/day
The second peak occurs during the mid-luteal phase at 250 micrograms/day.
2. During pregnancy, daily secretion is only 15-45 mg.
3. After menopause, daily secretion is low.
4. Before puberty, it is low and shows a rising trend.
In males, estrogen secretion is low, about 50 micrograms/day.
Average estrogen level: Oestrogen level in blood is low. In males, estrogen levels are significantly down and have no essential physiological functions.
In females
In males
Types
There are four endogenous estrogens with estrogenic hormonal activity.
1. Estrone E1 is more in serum during menopause. Estrone was isolated and purified in 1929 for the first time.
2. Estradiol E2 is more potent and prevalent than other types of estrogens. From menarchy to menopause, Estradiol E2 is the most important estrogen in females in the non-pregnant state.
3. Estriol E3 is the predominant estrogen during pregnancy.
4. Esterol E4 is secreted only during pregnancy.
Estradiol is the most potent estrogen, which is ten times as powerful as Estrone which is ten times as potent as Estriol.
Estradiol potency=10 times of Estrone.
Estrone potency =0 times estriol.
Minor endogenous estrogens are also synthesized, with some activity, and their physiological importance is not evident. All estrogens are synthesized from androgens, mainly testosterone and Androstenedione.
Mechanism of action
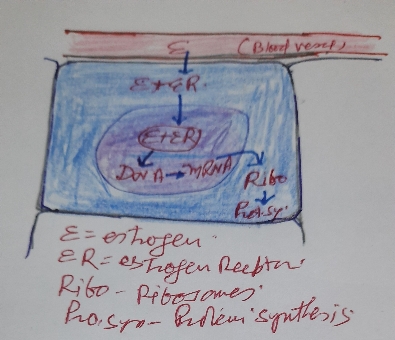
MECHANISM OF ESTROGEN ACTION
Steroid hormones readily diffuse passively across the cell membrane. Oestrogens being steroid hormones, rapidly diffuse across the cell membrane. Oestrogen enters all cells, but it has action only when estrogen receptors are present. It exerts effects mainly on the ovary, uterus, and breast. This is due to the presence of ‘estrogen receptors.
ER (estrogen receptor)is expressed in specific tissues, including the ovary, uterus, and breast.
In the cytoplasm, estrogens bind to and activate estrogen receptors. The Oestrogen receptor is a dimeric nuclear protein. Estrogen with estrogen receptors forms a complex that attaches to a specific DNA sequence to activate the transcription of target genes and promotes cell replication and protein synthesis. The DNA sequence is known as the ‘hormone response element.’
Estrogens are present at high levels in females of reproductive age and promote the development of ‘secondary sexual characteristics-for example, breast and endometrial thickening.
In males, estrogen is necessary for sperm maturation and essential for libido.
Before puberty, estrogen levels are deficient and exert little physiological effects.
At puberty, estrogen secretion increases and cause.
Causes growth of internal genitalia -ovaries, uterus, and vagina. It is responsible for the maturation and maintenance of the vagina and uterus.
It is responsible for ovarian cycle ovulation and corpus luteum formation.
Stimulates myometrial thickening.
Stimulates growth of the endometrium.
It increases vaginal wall thickness and increases vaginal lubrication.
Promotes external genitalia development-clitoris, labia majora, and labia minora.
It increases osteoblastic activities -bone formation, and decreases osteoclastic activities -bone resorption.
Increases binding protein synthesis by the liver.
Increases synthesis of coagulation factors and decreases antithrombin III.
Increases HDL and triglyceride and decreases LDL cholesterol. These effects prevent atherosclerosis and explain low Myocardial infarction in females.
Increases cortisol secretion and sodium and water retention.
Widening of hips.
Female fat distribution.
Essential for fertility.
Estrogens are neuroprotective -DNA repair.
Essential for mental health.
Transport
2-3% in free form in circulation is the active form of the hormone.
About 30% are bound to albumin and circulate.
About 68% are bound to ‘gonadal steroid binding globulin'( GBG) or ‘sex hormone binding globulin (SHBG).
Metabolism
Estrogens are metabolized mainly in the liver and, to some extent, In other tissues. Estrogens are conjugated in the liver with glucuronic acid to form water-soluble glucuronides and excreted in urine and bile.
Upon reaching the intestine, the bile portion is broken down by GUT flora and reabsorbed as active hormones. So in, liver diseases or disturbances in the gut flora alter this mechanism with disorders of menstrual cycles.
About’ learn-and fly.co.in’
These articles are part of my mission to provide trustworthy recent health information to support the general public, patients, and professionals worldwide.
Here you will find human physiology, anatomy, and health topics.
Summary
Estrogens are of four types – 1. Estrone 2. Estradiol 3. Estriol, and 4. Esterol
The primary female sex hormone is responsible for developing female genitalia and secondary sex characters.
Photo by – V.K.PRASAD
Hopefully, this article will be useful for you.
Follow me on Instagram.
And don’t forget to follow me on learn and fly .co.in.
I am more enthusiastic, and you can get new insights from my articles later.
Thank you.
FAQ :
Q. What does the estrogen hormone do?
A.Oestrogen acts on all parts of the body. In females, it is responsible for developing and maintaining reproductive organs and secondary sexual features. It is essential for mental health, the cardiovascular system, bones, and muscles.
In males, it is essential for libido and mental health.
Q. Types of estrogen?
A.
1. Estrone E1 is more in serum during menopause. Estrone was isolated and purified in 1929 for the first time.
2. Estradiol E2 is more potent and prevalent than other types of estrogens. From menarchy to menopause, Estradiol E2 is the most important estrogen in females in the non-pregnant state.
3. Estriol E3 is the predominant estrogen during pregnancy.
4. Esterol E4 is secreted only during pregnancy.
Estradiol is the most potent estrogen, which is ten times as powerful as Estrone which is ten times as potent as Estriol.
Estradiol potency=10 times of Estrone.
Estrone potency =0 times estriol.
Minor endogenous estrogens are also synthesized, with some activity, and their physiological importance is not evident. All estrogens are synthesized from androgens, mainly testosterone and Androstenedione.
Please submit any comments about the article Pancreatic function test. The team will work hard to evaluate the statement and make appropriate corrections.
This article discusses different aspects of testosterone -the male sex hormone. Here, learn about the site of secretion, average values, action, functions, and more…
Keywords: Testosterone| C 19 steroid| Leydig cells |testis |ovary estrogen| Luteinizing hormone | World Anti Doping Agency
Table of contents
1.
Introduction
2.
Site of secretion
3.
Biosynthesis
4.
Normal values and daily secretion
5.
Mechanism of action
6.
Functions
7.
Clinical
In males, testosterone is the primary sex hormone. In 1935, Ernst Laquer isolated, and Adolf Butenandt and Leopold Ruzicka synthesized testosterone.
Site of secretion:
Testis secretes testosterone from Leydig cells present in the seminiferous tubules. The testis also secretes estrogen in small amounts.
In females, ovaries secrete testosterone in lesser amounts.
Testosterone is synthesized by zona reticularis of the adrenal cortex.
Chemically testosterone is a C 19 steroid with one hydroxyl group in the seventeenth 17th position.
Biosynthesis of testosterone
Testosterone is secreted from cholesterol like other steroid hormones. Steps of synthesis:
The anterior pituitary gland’s Luteinizing hormone (LH) controls testosterone secretion.
The Luteinizing hormone stimulates the Leydig cells via c AMP. The mechanism is as follows.
c AMP coupled to Gs triggers many reactions causing the formation of testosterone.
c AMP
Average plasma concentration depends on age and sex, in
Adult male-300-1000 ng[i]/dl of blood. It decreases with advancing age. Testosterone is used in older men to fulfill the deficiency. and
Adult females have 30 to 70 ng/dl of blood.
Daily secretion of testosterone varies in males and females.
In adult males average is 7 mg per day, and in females, it is 300 micrograms per day.
The physiologically active form of testosterone circulates in the free state, only 1-2%.
97-98 % of testosterone circulates bound to plasma proteins.
About 65% binds with GBG -gonadal steroid binding globulin and 33 % with albumin, rest to other plasma proteins.
Mechanismofaction:
Cells of target organs have specific receptors for testosterone. Testosterone combines with these receptors, and inside the cell, it is converted into dihydrotestosterone by 5-‘alpha reductase’.
Dihydrotestosterone is active and enters the nucleus, which binds to nuclear chromatin and stimulates mRNA .Stimulated m-RNA stimulates protein synthesis.
Metabolism and excretion:
The liver inactivates dihydrotestosterone into androsterone and dehydroepi androsterone., conjugate it with glucuronic and sulphuric acids as 17-ketosteroid .17-ketosteroids are excreted in the urine.
Functions:
In males,testosterone is responsible for :
Loss of virility and fertility due to loss of testis has been known since antiquity.
1. Development of male reproductive tissues-testes, prostate.
2. Development of secondary sexual features-increase in bone mass, muscle mass, and increased hairs.
In both sexes, testosterone is responsible for
1. Good mental health and well-being.
2. Prevention of osteoporosis.
Detail of functions:
1. Maintenance of Spermatogenesis.
2. Promotes and maintains the motility of the sperms.
3. Promotes and maintains the fertilizing capacity of the sperm.
4. Causes development of accessory sex organs and secondary sexual features at puberty -penis and scrotal enlargement.
5. Testosterone plays a crucial role in adolescent growth spurts and increases libido.
6. Testosterone has an anabolic effect-increases muscle mass, and increases muscular strength.
7. Testosterone has virilizing and anabolic effects.
8. Testosterone regulates acute hypothalamic-pituitary-adrenal axis responses when there is a dopaminergic challenge.
9. Testosterone regulates thromboxane A2 receptors on the megakaryocytes and platelets, regulating platelet aggregation.
10. Masculinization of the male child’s brain occurs at 4 to 7 months by transforming testosterone into estrogen, which crosses the blood-brain barrier and enters the male brain.
Female brains are not affected as female fetuses have alpha-fetoprotein, which binds the estrogen so that the estrogen can not pass the blood-brain barrier.
Testosterone is used in the treatment of
Hypogonadism in men
Breast cancer in women.
To increase muscular strength in athletes, it is ‘prohibited for all times’ by the World Anti Doping Agency”.
The older age group is sometimes used to fulfill the reduced testosterone level.
Clinical
Comparison of effects of low testosterone in males and females
Sr.no.
Effects of low testosterone in males
Effects of low testosterone in females
1.
Loss of libido
loss of libido
2.
Low muscle mass and strength Lack of body hair Slowed growth of secondary sexual characteristics Erectile dysfunction Infertility Delayed puberty
Infertility Menstrual disorders Amenorrhea
3.
Depression
Depression
4.
Cognitive disorders
Cognitive disorders
5.
Insomnia
Insomnia
6.
Lack of motivation
Lack of motivation
Effects of low testosterone in males include
Loss of libido
Low muscle mass and strength
Lack of body hair
Slowed growth of secondary sexual characteristics
Erectile dysfunction
Infertility
Delayed puberty
Depression
Cognitive disorders
Insomnia
Lack of motivation
Effects of low testosterone in females include
Loss of libido-sex drive
Infertility
Menstrual problems
Depression
Insomnia
Lack of motivation
Comparison of low testosterone in males and females:
Sr.no.
Causes of low testosterone in males
Causes of low testosterone in females
1.
Testicular failure due to trauma, viral infection
Old age
2.
Pituitary tumor or disease
Ovarian failure
3.
Hypothalamic tumor or disease
Oral contraceptive -long-term use.
4.
Chronic diseases such as diabetes mellitus
Chronic diseases such as diabetes mellitus
Causes of low testosterone in males include
Testicular failure due to trauma, viral infection
Pituitary tumor or disease
Hypothalamic tumor or disease
Chronic diseases such as diabetes mellitus
Some genetic diseases
Causes of low testosterone in females include
Old age
Ovarian failure
Oral contraceptive -long-term use.
Now, treatment of low testosterone is available for both males and females, known as ‘testosterone replacement therapy (TRT)’.-
Topical gel,
Patches
Testosterone injectable
Testosterone implant
Organ transplant in males -under trial.
Effects of high testosterone in males include
Excessive body hairs
Well-developed muscles and sexual organs.
Causes of high testosterone in males include
Adrenal hyperplasia
Tumors of the testis or adrenal cortex
Drugs.
Effects of high testosterone in females include
Hirsutism -Excessive body hair in male fashion.
Virilization -masculine appearance, deep voice, etc.
Causes of high testosterone in females include
Ovation tumor
adrenal gland tumor
polycystic ovarian syndrome
drugs- estrogen, clomiphene.
About’ totalphysiology.com.’
I aim to provide trustworthy recent health information to support the general public, patients, and professionals worldwide through these articles. This is my passion.
Here you will find human physiology, anatomy, and health topics.
Summary
The primary male sex hormone is testosterone, secreted mainly by the testis and, to some extent, by the zona reticularis of the adrenal cortex. In females, it is also secreted by the ovaries (though in little amount ) and zona reticularis.
In males, it is responsible for the development of male reproductive tissues-testes, prostate, and secondary sexual features-increase in bone mass, muscle mass, and increased hairs.
In both sexes
Testosterone is responsible for good mental health, well-being, and the prevention of osteoporosis.
FAQ :
Q. How to increase testosterone levels naturally?
A. Here are some natural methods to increase testosterone in both genders: lifestyle, change-Exercise, balanced diet at regular intervals, rest, no tension, or at least minimize stress in males, protect scrotum from trauma, infection, and exposure to high-temperature occupational hazards.
Q. How can you tell that a woman has a high testosterone level?
A. Effects of high testosterone in females include
Hirsutism -Excessive body hair in male fashion.
Virilization -masculine appearance, deep voice, may become bald.




Leave a comment