Introduction:
Blood circulation in the arteries and veins that supply the heart is known as ‘coronary circulation.’ The heart contains and supplies blood but cannot use it directly.
Table of contents:
- Introduction:
- The coronary arteries:
- Normal anastomosis:
- Functional anastomosis
- Coronary Sinuses:
- The great cardiac vein
- Chemical factors:
- Neural control
The heart is unique in nature, and it can not rest. Its primary function is to pump blood. The heart has three layers- epiderium, myocardium, and endocardium. The myocardium remains between the two layers and performs the primary function of pumping blood.
Blood comes through arteries to the heart muscle and its layers and leaves through veins.
As we have seen, it is a very active organ that needs a sufficient supply of oxygen and nutrients and the rapid removal of metabolic waste.
Arterial blood supply:
The coronary arteries:
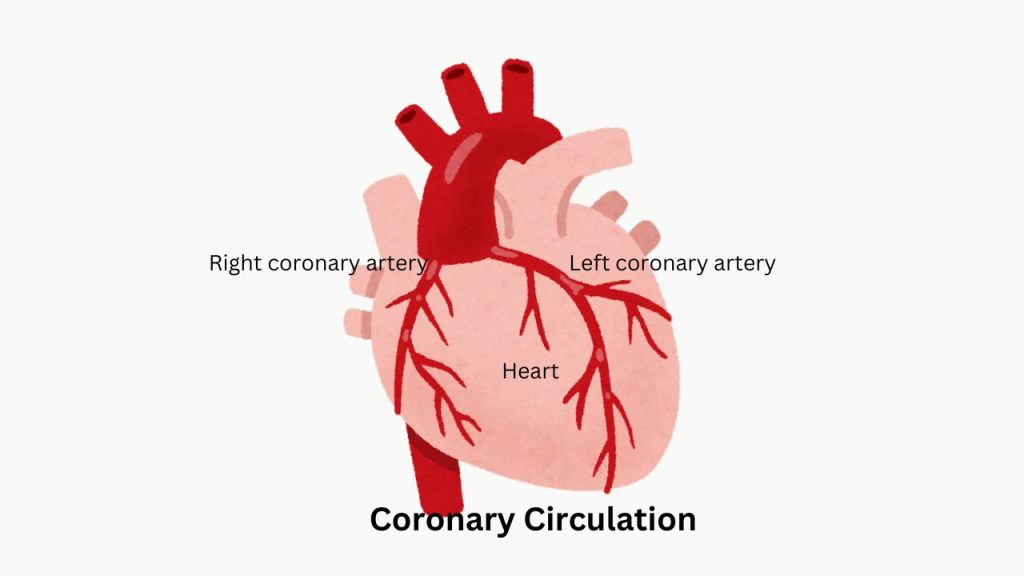
Two coronary arteries supply the heart. The blood supply of the heart is by two coronary arteries; they are
1. Right coronary artery and
2. Left coronary artery.
Functional anastomoses:
1. Cardiac anastomoses
2.Extracardiac anastomoses
Venous drainage :
1. Superficial veins
1. Right atrium
2. Deep veins
We will now discuss the right and left coronary arteries, which arise from the aorta’s root to supply blood to the heart.
Right coronary artery
The right coronary artery is posteriorly in the right Atrioventricular sulcus and gives an acute marginal branch. Before anastomosis with the left coronary artery, it provides many descending branches. The right coronary artery mainly supplies the following parts or portions of the heart.
The right coronary artery supply:
2. Major part of the right ventricle and interventricular conducting system of the heart.
3. Posterior part of the interventricular septum and an adjacent small portion of the left ventricle.
4. Sinoatrial (Pacemaker of the heart) and Atrioventricular nodes.
Left coronary artery
The left coronary artery is present anteriorly in the left atrioventricular sulcus. It supplies only 20% of the heart.
It is divided into:
1. Anterior descending branch, which is present in the interventricular groove. Therefore, it is also known as the ‘anterior interventricular branch’ and has many septal branches.
2. The left circumflex artery continues in the A-V groove and proceeds downwards as posterior descending branches. It anastomoses with the right coronary artery.
The areas supplied by the left coronary artery:
1. Left atrium
2. Major part of the left ventricle and left branch of the “bundle of His.”
3. Anterior part of the interventricular septum and adjacent small portion of the left ventricle.
The coronary arteries are end arteries.
Anastomosis
Normal anastomosis:
In normal conditions, numerous anastomoses occur between the branches of coronary arteries, and some remain dormant.
Functional anastomosis
Functional anastomosis: in ischaemic conditions, functional anastomosis of two types becomes apparent-
- Cardiac anastomosis between branches of coronary arteries.
- Extracardiac anastomoses between :
i. Vasa-Basora of the aorta and pulmonary arteries.
ii. Intrathoracic, bronchial, and phrenic arteries.
Deoxygenated blood goes into veins.
Venous draining
1. Veins present beneath the epicardium
Coronary Sinuses:
Mainly drains the myocardium supplied by the left coronary artery. It drains in the posterior wall of the right atrium.
The great cardiac vein
The great cardiac vein drains the left ventricle’s myocardium and the coronary sinus.
The anterior cardiac vein drains the myocardium supplied by the right coronary artery. It is located in the anterior wall of the right atrium.
2. Veins are present in the deep myocardium
Veins present in the deep myocardium directly open in the cardiac chambers.
Arterio sinusoidal, arterio luminal, and Thebesian vessels into the left heart. Therefore, pO2 is 98%, slightly less than 100%.
Oxygen consumption:
The heart consumes a lot of oxygen, and this consumption changes with activity. At rest, myocardial oxygen consumption is 60 to 80 ml per 100 gm per minute, increasing fourfold during exercise. This is regulated by autoregulation and nervous and chemical factors.
Usually, the oxygen supply does not exceed the myocardial need. If the myocardial demand exceeds the oxygen supply, a mismatch produces myocardial ischemia or infarction.
The heart operates only in aerobic conditions, so myocardial oxygen consumption is very high. The left ventricle’s oxygen consumption is about 25 ml/minute, or 10% of the whole body’s.
Chemical factors:
Chemical: Chemical control plays an essential role in the coronary circulation. Nervous control plays a minor role in the coronary circulation.
Intracellular myocardial ‘adenine nucleotides’ are converted into ‘adenosine,’ which diffuses into the extracellular fluid when the heart receives less blood. Adenosine is a potent coronary vasodilator.
Increased heart activity produces carbon dioxide, hydrogen ions, potassium ions, lactic acid, and adenosine. These metabolites produce coronary vasodilation, which increases blood supply to the heart.
Nitrates increase coronary blood flow.
Hormones –Thyroid hormones, epinephrine, nor-epinephrine cause an increase in the coronary circulation.
Neural control
Neural control: Nervous control plays a minor role in coronary circulation.
Clinical
Causes of myocardial ischemia and infarction,
Usually, the oxygen supply does not exceed the myocardial need. If the myocardial demand exceeds the oxygen supply, a mismatch produces myocardial ischemia or infarction, as seen in vigorous exercise or physical work.
Coronary blood circulation may be interrupted for many reasons, including embolism and coronary artery diseases.
Hashtag:Autoregulation#End arteries #oxygen#consumption# coronary artery#Adenosine#Venous drainage#
FAQ:
Q1. What are end arteries?
A. When an artery supplies blood in a given area of an organ, there is no overlap of blood supply. If this artery is blocked for any cause, the area supplied by it will become ischaemic, and later, it will be necrosed.

Leave a comment